
Shock reduction using ATP as 1st line therapy for spontaneous sustained ventricular tachycardia in patients with ischemic dilated cardiomyopathy and severly depressed ventricular function
Posted: September 26, 2014 Filed under: eHealthCare, Medical Devices, Professionnal guest Leave a commentAuthors: Stefano Nardi MD, PhD (*), Luigi Argenziano MD, PhD (*)
(*) Arrhythmia, Electrophysiologic Center and Cardiac Pacing Unit, Thoracic Surgery and Cardiovascular Department, Presidio Ospedaliero Pineta Grande, Castel Volturno (CE), Italy (I)
Introduction
Implantable cardioverter-defibrillators (ICDs) have clearly demonstrated to terminate an elevated percentage of sustained ventricular tachycardia (SVTs), both with shock therapy and, painlessly, with antitachycardia pacing (ATP). The purpose of this study was to investigate the efficacy and safety of ATP as 1st line therapy for terminating SVTs, occurring in patients (pts) with coronary artery disease (CAD) and severely depressed left ventricular ejection fraction (LVEF) due to not reversible causes, comparing this approach with shock.

Figure 1: Rationale for ATP Rx is that a “WAVE-FRONT” critically temporized with VTCL and applied proximal to the “Slow Conduction Zone” is able to capture the CIRCUIT, then interrupt the reentry
Methods
From March 2004 through June 2013, 408 consecutive patients (pts) were considered eligible for this study, according with MADIT and/or SCD-HeFT criteria, and 387 of them (94,8%) accepted and underwent ICD implant. Pts were randomly assigned to ATP group (190/387) or shock group (197/387) and three zone of detection were assigned in all pts: a slow VTs window (320-400 msec), a fast VTs window (240-320 msec), and a ventricular fibrillation (VF) window (<320 msec). In ATP group, 3 burst sequence were programmed in slow VT zone and 1 burst sequence was programmed in fast VTs zone (burst sequences of 8-10 pulses at 88% CL) before shock, respectively, whereas in shock group (87/169) shock was adopted as 1st line therapy for all SVTs. No statistically differences, in term of age (72,2 vs 73,4, p=NS), sex (man 73,1% vs 69,3%, p=NS), NYHA functional class (2,8 vs 2,6, p=NS), LVEF (24,5% vs 26,9%) and drugs therapy were observed between two groups. Based on the evaluation of stored electrograms (EGMs), we aimed to prospectively follow pts and to analyze these two different therapeutic approach.

Figure 2: ATP programmability with adaptative cycle length
Results
A total of 3,288 spontaneous VTs episodes occurred in 171 pts (41,9%) during a mean follow-up of 54,4±23,1 months (90 pts in ATP group and 81 pts in shock group). Among these, 2,235/3,288 (67,9%) were SVTs and 612 of them (27,4%) were detected in VF zone, and then treated with primary shock delivery, whereas in the remaining 1,623 of them (72,6%), 936 episodes occurred in ATP group (57,6%) and 687 episodes occurred in shock group (42,4%). In ATP group, ATP was able to terminate successfully 80,7% of SVTs, failed in 9,3% of SVTs, finally reverted by shocks, and in 10% of SVTs ATP was able to converted arrhythmias in a slower VT, outside the VT zone. 61% of these slower SVTs were self-terminating whereas 39% were redetected and treated. Finally, in primary intention-to-treat basis, ATP was successful in 834/936 SVTs (89%) and unsuccessful in 102/936 SVTs (11%). In contrast, 657/687 (95,6%) of all SVTs episode detected in VT zone and that occur in shock group were shock terminated, whereas 30/657 (4,4%) were accelerated into VF zone. The individual termination rate and acceleration rate per pt were comparable in both groups, as well as mean time of SVT termination (ATP=12.6 sec vs Shock=10.9 sec, p=NS).

Figure 4: Results of a registry comparing ATP vs shock therapy as primary choice of VT treatment for a total of 387 pts enrolled
Conclusions
Our data suggest that ATP is a safe and effective therapeutic approach for SVTs termination, also in pts with DCM and very depressed LVEF; then, this therapeutic approach should be programmed “on” in all patients regardless LVEF.
Authors: Stefano Nardi MD, PhD (*), Luigi Argenziano MD, PhD (*)
(*) Arrhythmia, Electrophysiologic Center and Cardiac Pacing Unit, Thoracic Surgery and Cardiovascular Department, Presidio Ospedaliero Pineta Grande, Castel Volturno (CE), Italy (I)
Cardiac conduction disturbances : the other side of sudden cardiac death in hypertrophic cardiomyopathy.
Posted: October 21, 2013 Filed under: Medical Devices, Professionnal guest | Tags: arrhythmias, atrio-ventricular block, AVB, cardiac, cardiac conduction disturbances, cardiac death, cardio, cardiomyopathy, CCD, HCM, hypertrophic, Hypertrophic cardiomyopathy, myocardial, sudden, sudden cardiac death, tachy-arrhythmias, ventricular Leave a commentCardiac conduction disturbances: the other side of sudden cardiac death in hypertrophic cardiomyopathy.
Hypertrophic cardiomyopathy (HCM) is a myocardial disease characterized by asymmetrical hypertrophy of the heart and disarray of myocardial cells, with an unstable electrical substrate potentially causing lethal ventricular tachy-arrhythmias 1.

Cardiac magnetic resonance imaging (short axis view) of a patient affected by HCM
Sudden cardiac death is the worst feared complication of hypertrophic cardiomyopathy (HCM), and is known to be mostly related to ventricular arrhythmias such as ventricular fibrillation and ventricular tachycardia 1. However, arrhythmic sudden cardiac death can also be related to cardiac conduction disturbances (CCD), including complete atrio-ventricular block (AVB), possibly leading to prolonged asystolia. The only available treatment for such CCD, is the pacemaker (PM).
Third degree atrio-ventricular block.

Red arrows: QRS (ventricular electrical activity). Black arrows: P waves (atrial electrical activity).
Atrial and ventricular activity is completely dissociated.
Second degree advanced atrio-ventricular block.

Red arrows: QRS (ventricular electrical activity). Black arrows: P waves (atrial electrical activity).
Consecutive P waves care not followed by QRS, leading to a transient asystolic pause.
Although CCD are commonly seen in association with amyloidosis and glycogen storage disorders, which may themselves be associated with left ventricular hypertrophy 1, little is known about the prevalence of primitive CCD in HCM.
Primitive CCD
Case reports.
A few case reports of HCM patients with complete primitive (i.e. not secondary to surgicalor interventional procedures) AVB have been reported.
Paroxysmal complete AVB has been described in three HCM patients, with prolonged QRS duration at ECG, suffering from recurrent attacks of syncope and cardiopulmonary arrest 2. Symptoms were likely related to the AVB itself.
A case of a north Indian family including nine HCM individuals, among whom 5 underwent PM implantation due to advanced AVB at an age of 39-55 years, has also been described 3. Two sudden cardiac deaths (25 and 51 years of age respectively) were also reported in the same family. The absence of CCD in all the HCM-affected members of the family (therefore sharing the same genetic mutation, likely associated with CCD), may be explained by the phenomenon of incomplete “penetrance” (i.e. the proportion of individuals with the mutation who exhibit clinical symptoms), which in turn is influenced by several factors, including age and gender.
Clinical studies
Prospective studies investigating the prevalence of CCD in HCM requiring permanent PM implantation are lacking. In a retrospective analysis of a small cohort of HCM patients (27 patients; 12 non obstructive) with an implanted PM, a high rate of AVB was observed4. Indications for PM included: spontaneous or induced AVB in 54% of cases (with spontaneous total AVB in over 15% of cases) and support for drug-induced bradycardia in 8% of cases 4.
A larger retrospective study of 451 HCM-patients (44% with previous syncope), also reported a high prevalence of CCD. Overall, PM was implanted in 11% of patients, either due to sinus node dysfunction or to AVB. Interestingly, in 18% of cases, at least one other family member was a PM recipient. One single mutation (E101K in the cardiac actin gene) was identified in 3 index cases (PM recipients). The authors concluded that CCD may form part of the phenotype expression of HCM and may have a familial component 5.
Iatrogenic CCD
Obstruction of the LV outflow tract in HCM, due to septal hypertrophy, is dynamic and varies with loading conditions and contractility of the left ventricle. Interventional procedures for reduction of the left ventricular outflow pressure gradient, such as septal alcohol ablation (SA) or surgical septal myectomy (SM) can be complicated by a not negligible rate of CCDs.
Septal ablation
Trans-catheter alcohol embolization of selected branches of the coronary arteries, aims at generating a circumscribed septal infarction of the left ventricle, in an attempt to reduce the left ventricular outflow tract pressure gradient due to loss of myocardial contraction. The iatrogenic septal infarction usually extends between the anterior and inferior free walls of the left ventricle, in an area commonly containing the right bundle branch (RBB) of the conduction system. Septal Ablation is therefore often complicated by RBB block occurrence 6. AVB has also been described in up to 62% of cases of SA, but is usually transient and characterized by a spontaneous regression within 24 hours. The frequency of CCDs following SA which require permanent PM implantation has ranged between 10% and 33% across studies 6.
Subacute AVB have been also been described, occurring up to 8 days after SA 7. Predictors of subacute AVB post-ASA include: advanced age, prolonged QRS duration before or after SA, new intra-ventricular conduction disturbances or first-degree AV block after SA 7.
Septal myectomy
Septal myectomy entails surgical removal of sub-endocardial tissue in the anterior inter-ventricular septum in an attempt to reduce ventricular contractility and left ventricular outflow tract gradient. Since the left bundle branch fibers of the cardiac conduction system are adjacent to the anterior inter-ventricular septum, patients undergoing SM are at increased risk of developing left bundle branch block. Interestingly, CCDs have been shown to be significantly lower following SM as compared with SA 6,8. The risk of complete AVB is approximately 2% with SM (higher in patients with preexisting RBB block 1 .
Considerations
Current guidelines underline the importance of PM implantation when an advanced CCD occurs after SA or SM 1. However, in planning a PM implantation due to AVB in a HCM-patient, a few considerations must be taken into account, including:
- eventual benefits expected from pacing of the right ventricular apex, in terms of reduction of the left ventricular outflow tract gradient and consequent symptoms reduction1;
- the individual risk of tachy-arrhythmias eventually precipitating sudden cardiac death, with possible indication for cardioverter defibrillator implant.
Nowadays, the availability of sophisticated high-quality PM, such as those provided by NayaMed, allows safe and efficient protection from CCD and associated risk of sudden cardiac death in HCM individuals.
Dr. Annamaria Martino, Dr. Lucia De Luca and Prof. Leonardo Calò
Cardiology Department, Policlinic Casilino, ASL RMB, Rome, Italy.
References
- Gersh J. et al. 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2011; 58:e212-260
- Doven O et al. Abnormal His- Purkinje system conduction leading to complete atrioventricular block in patients with hypertrophic cardiomyopathy: a report of 3 cases. Jpn Heart J. 2004;45:347-52.
- Bahl A, Nahar Saikia U, Talwar KK. Familial conduction system disease associated with hypertrophic cardiomyopathy. International Journal of Cardiology 2008; 125: e44–e47
- Alves Silva LA et al. Cardiac Pacing in Hypertrophic Cardiomyopathy. A Cohort with 24 Years of Follow-Up. Arq Bras Cardiol 2008;91:250-256
- Barriales-Villa R et al. Severe cardiac conduction disturbances and Pacemaker implantation in patients with hypertrophic cardiomyopathy. Rev Esp Cardiol. 2010;63:985-8
- Agarwal S et al. Updated meta-analysis of septal alcohol ablation versus myectomy for hypertrophic cardiomyopathy. J Am Coll Cardiol 2010;55:823–34
- Lawrenz T et al. Predictors of complete heart block after transcoronary ablation of septal hypertrophy: results of a prospective electrophysiological investigation in 172 patients with hypertrophic obstructive cardiomyopathy. Am Coll Cardiol. 2007;49:2356-63.
- Talreja DR et al. Alcohol septal ablation versus surgical septal myectomy: comparison of effects on atrioventricular conduction tissue. J Am Coll Cardiol.2004;44:2329-32.
NayaMed Cool.Cast – Topic 1 – AT Management
Posted: January 7, 2013 Filed under: Uncategorized Leave a comment
At NayaMed, we realize that you have an endless number of choices of what to read on the internet, especially as they relate to medical devices. Therefore, I’d like to say thank you for landing here, on the NayaMed blog to learn more about the AT Management Cool.Cast series.
So, why did we launch the new Cool.Cast Series with AT Management? It’s simple; the incidence of Atrial Fibrillation (AF) is growing at an alarming rate. Our Technical Advisors can personally attest to, and have seen first-hand, that devices can be utilized by clinicians to detect subclinical and symptomatic AF, thus helping to address this growing problem. Before continuing, I believe it’s important to explain that our AT Management Cool.Cast Series will not teach you how to manage your AT device patients, you know this far better than we do. What our AT Management Cool.Cast Series will do, is to strangely entertain and uniquely train on the AT Management features in NayaMed devices.
The first delivery of the AT Management Cool.Cast Series is an infographic, ‘A look at the evolution of medical devices & equipment in the past century’. You may have already seen it and if so, we hope you enjoyed the ‘experience’. We encourage you to pin it, post it, print it, tweet it, blast it, read it again and again….there are no rules so why not have some fun.
The second delivery of the AT Management Cool.Cast Series is a Tech Tip called ‘Better Diagnosis of Atrial Flutter & Atrial Fibrillation in NayaMed Pacemakers’. I think you’ll find that our Tech Tips are a fast and simple way to learn about NayaMed devices. In fact, after reading our AT Management Tech Tip, we believe you’ll say to yourself, sure, this is something that I can keep in the back of my mind for my AT patients.
The final delivery of the AT Management Cool.Cast Series is a NayaCast titled ‘Blanked Flutter Search’. With this video simulation, we explain an AT feature that is, in our opinion, not wholly appreciated and maybe even sometimes misunderstood. We’re confident, though, that after experiencing the ‘Blanked flutter Search’ NayaCast you’ll see that the feature is actually quite smart and an important one to have in a device for your AT/AF patients.
Now that you know what to expect from our AT Management Cool.Cast Series, I don’t think I’d be doing a thorough job if I didn’t describe all of our AT Management features – AT is the topic after all.
So, without further ado, here are the AT Management features that can benefit patients with AT/AF:
- Mode switch which, when coupled with Blanked Flutter Search, allow patients with regular Atrial Flutter, or AF, to appropriately mode switch. Seems like a normal thing to have but not everyone has this!
- Conducted AF Response (CAFR) which regularizes the ventricular rhythm during an AT/AF episode and thus aims to minimize the symptoms of an irregular rhythm due to AT/AF. Again, a nice feature to have in your back pocket for those patients that are symptomatic from an irregular rhythm due to AT/AF.
- High Rate Episodes Collected Data to help identify true AT/AF as early as possible. Our Tech Tip talks about how to use and interpret the results in your AT patients.
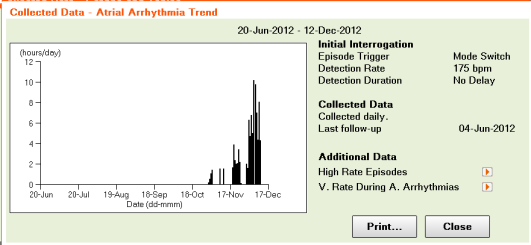
- Atrial Arrhythmia Trend to help determine the time spent each day in an AT/AF and over time.
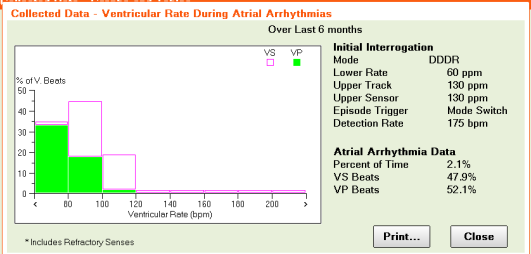
- VRate During AT/AF Histogram to help determine whether the ventricular rate is controlled while in AT/AF.
- Non-competitive atrial pacing (NCAP) to prevent pacing during the atrial vulnerable period, which could induce an AT/AF episode. Not a game changer but again, good to have.


So, with this blog post, we kick off our Cool.Cast Series with AT Management.
Mary Soranno
NayaMed Technical Advisor
Audible alerts or How to make the ICD more efficient and the patient safer
Posted: November 22, 2012 Filed under: Medical Devices | Tags: Audible alerts, ICD, RV Lead Integrity Alert, RV pacing lead Leave a commentAn ICD is saving lives. It gives peace of mind to our patients thinking that at any moment, if their heart stops “someone” will be there to “bring it back”. Taking in consideration that most people who experience a sudden cardiac arrest do not survive the first event, the ICD is one of the great medical inventions of the 20th century.
In order for the ICD to treat the ventricular arrhythmia it needs to accurately detect them. Undersensing and Oversensing are the two significant problems affecting the detection in an ICD.
There are also 2 categories of situations in which the patient should be notified: if his clinical condition is getting worse and if the system’s functionality is in danger. In big majority of cases the ICDs are reliable devices but, sometimes a part of the system can break and in those moments it is extremely important to warn the patient immediately in order for him to contact his physician as soon as possible. This is particularly true when the integrity of the defibrillation lead is threatened.
Soon after the implantable defibrillator became the 1st line of defence against the SCD, physicians realised the inappropriate therapies are the biggest complication.
Getting an ICD is an important moment in a patient’s life and for primary prevention it is something difficult for the patient to understand “Why do I need a device when I never had a cardiac arrhythmia before?” Now, imagine this patient after getting his primary prevention ICD starting a home activity where he is using his arm a little more than before, like playing tennis with his son. Imagine that after a few days he starts receiving inappropriate shocks. He’s been told the ICD is there to save his life but in exchange he’s passing in pain because of it. This is just an unfortunate event but it is the reason why in NayaMed we have implemented a number of clinical and device alerts specifically designed to warn the patients about potential problems.
The ICD leads are complex medical devices and all the manufacturers are seriously testing them before the market release but with all this, a problem can appear. In those situations the NayaMed ICD will start ringing an alarm at constant intervals and it is among the only devices in the market that will ring daily, until a physician is checking the device.
As the right ventricular lead problems represent the major complication in the ICD, NayaMed has 3 separate analysis and alerts aiming to detect a possible RV lead problem.
The constant impedance check is the classical alert that will ring if the impedance value goes out of certain ranges, but NayaMed ICD can do much more…

The Lead Integrity Alert is probably one of the most ingenious and useful alerts on the market. It is monitoring the important variations in the lead impedance, the short not-physiological ventricular intervals (close to the ventricular blanking) and highly rapid non-sustained ventricular events (that could be due to a lead rupture and not to real heart contractions). It integrates the information from those 3 parameters in the following way:
- An RV pacing lead impedance measurement is less than 50% or greater than 175% of the baseline impedance. The baseline measurement is the median of the previous 13 daily measurements.
- The ventricular Sensing Integrity Counter is incremented by at least 30 within a period of 3 consecutive days or less.
- The device senses 2 High Rate-NS episodes with a 4-beat average R-R interval of less than 220 ms.
If at least 2 of the following criteria have been met within the past 60 days, it identifies a potential lead fracture.

When the criteria for the RV Lead Integrity Alert are met, the device immediately sounds an alert tone. The tone sounds again every 4 hours beginning at the next scheduled 4-hour time interval. The tone also sounds at the programmed Alert Time and when a magnet is placed over the device.
What is important is in the NayaMed ICD, the tone continues to sound until the device is interrogated by a programmer.
Using this alert, in case of a lead fracture, the patient will receive a 3 days warning* before the inappropriate shocks start. As mentioned in the graph, it is not a simple alert but it also takes some proactive actions to minimize the consequences of a broken lead and help to diagnose it.
![]()
One of the newest alerts on the device market is the RV lead noise which is actually differentiating between noise and a real VT/VF event. When VT/VF detection is withheld due to lead noise and the RV Lead Noise Alert is on, the device sounds a patient alert tone. This tone then sounds every 4 hours beginning at the next scheduled 4-hour time interval. The alert tone also sounds at the programmed Alert Time and when a magnet is placed over the device.

The Important aspect… the alert tone continues to sound until the device is interrogated by a programmer. As the previous one, it is not only an alert but also a discriminator preventing the inappropriate shocks due to noise.
VF Detection or VF Therapy OFF, low battery voltage and the excessive charge time are also 3 alerts warning the patient that he/she should consult his physician as soon as possible.
All the device alerts are nominally switch ON so basically we can say that if the system has a hardware problem… the patient will be notified.
The physician also has the possibility to program the alert time in respect with patient preferences and activity.
![]()
In addition to those important device alerts there are 2 clinical alerts helping the physicians to better manage the patients; in case the number of shocks delivered in a VT/VF episode is greater than or equal to the programmed Number of Shocks Threshold and if a specific VF, VT, or FVT episode was redetected after all programmed therapies for that type of episode were delivered.
All the alerts can be easily programmed from the Alert button on the Parameter screen.

Analysing all those aspects we’re happy to say that the NayaMed ICD has probably one of the biggest range of audible device alerts that will constantly monitor the system and ring when necessary. They work not only with the NayaMed leads but with any compatible lead on the market making the ICD a better lifesaver.
*Swerdlow CD, Gunderson BD, Ousdigian KT, Abeyratne A, Sachanandani H, Ellenbogen KA. Downloadable Software Algorithm Reduces Inappropriate Shocks Caused by Implantable Cardioverter-Defibrillator Lead Fractures. A Prospective Study. Circulation. Published online September 27, 2010.
Alexandru Trif
Technical Reps…
Posted: October 23, 2012 Filed under: Medical Devices 3 CommentsNayaMed launched RTS (Remote Technical Support). What is it? For people who don’t know the medical device industry allow me to explain it:
For people who don’t know the medical device industry allow me to explain it:
It occurs, when a healthcare provider (Hospital) has to implant a pacemaker or defibrillator, a technical engineer representing the company of the implantable medical device is assisting the procedure. This is happening
less for a pacemaker but most of the times for a defibrillator. What is he doing? When, regarding pacemakers and defibrillators, most of the time, nothing than being there.
He is a kind of insurance or advisor. He is ready to answer questions that the clinical staff might have.
Now if you think about the number of pacemaker or defibrillator implants that happen in Europe, you keep that number, taking out 20%, and you end up with the number of presence time of technical reps. I did the math. It is amazing.
Back to the genesis of NayaMed, we decided to change this because, said or not, there is a cost behind this traditional best practice. It is a cost that could have a better value for customers particularly for implanters.
RTS is a solution that provides healthcare providers with technical support online during the implant. It means a centralized team of the best technical advisors can be reached just by pressing on a button.
How does it work? We did develop equipment (RTS Box) that is plugged into the programmer and at the same time connected to the internet. By using a headset, the press of a single button initiates a call with a dedicated technical advisor that is able to see the programmer screen.
Hold on for a minute and think about it…… Think about the large scale impact of this. Think about the use of this box for implant or follow-up. Think about an implanter. Instead of disturbing him during his lecture 50km away from his hospital, his staff can just connect the RTS Box and get in touch with a high knowledgeable technical advisor. Think about training of the staff. Think about the “Anytime – anywhere”…. Are you getting it?
I remember at the beginning some people told me: “noway, you are removing a guy from the cath lab; a guy that helps during the implant; two hands gone….that won’t work”. Well I was naïve and concerned about this. But after many discussions with numerous implanters all over Europe, they almost all confessed, they could renounce at the presence of a Technical Consultant in the OR during the implant procedure. Moreover they realised the presence of the TC is sometimes a waste of resources. The RTS solution combined with an eLearning program could be the perfect solution for making the Implant center autonomous and economically more efficient.
Today NayaMed is rolling out RTS Boxes everywhere. Implanters start to welcome us with a very interesting look…..some are just waiting for us.
www.nayamed.com allows pre-booking of technical advisors and getting the paperwork done more easily.
 In a near future I believe medical device companies will come up with alternative solutions or even collaborating with our solution. That day, I will be proud and happy, we will all be proud. It will mean NayaMed will have achieved one of its objectives…..
In a near future I believe medical device companies will come up with alternative solutions or even collaborating with our solution. That day, I will be proud and happy, we will all be proud. It will mean NayaMed will have achieved one of its objectives…..
Frederic Briguet
Head of eBusiness and Marketing
NayaMed
Thank you for visiting us at the ESC Congress 2012 in Munich
Posted: September 10, 2012 Filed under: NayaMed spirit | Tags: bradycardia, cardiac electrophysiology, cardiac techniques, congress, eHealthcare, ESC, Germany, Health 2.0, healthcare organizations, ICD, Medical Devices, Munich, pacemaker, pacemakers, video 4 Comments
NayaMed products in a few words
Posted: August 20, 2012 Filed under: Medical Devices | Tags: bradycardia, cardiac, cardiac electrophysiology, cardiac techniques, cardiology, conventional devices, defibrillator, eHealthcare, Health 2.0, ICD, Medical Devices, pacemaker, pacemakers, St Jude Medical, technical advisor Leave a commentAs a new appearance on the CRDM Market, customers often ask: “Who are you NayaMed?”, “What are your products and why should we chose you for our patients?”
Well, mostly because we offer a simple online platform with a permanent access to your products, giving full transparency and allowing permanent access to ordering, digital inventory, stock management access and technical support.
Also, because as a clinician, you get the product you need when you need. A product that has been designed and engineered to perfectly match the NayaMed philosophy – Smart and Simple.
We wanted the clinicians to be comfortable when using our devices, so we asked our Technical Advisors to present the NayaMed products in just a few minutes.
Mary Soranno and Marina Mancusi, our technical advisors for the UK and the Italian market did a wonderful job and we are inviting you to see a very brief, but complete presentation of our products in English or Italian.
English Version:

Italian Version:

NayaMed devices made simple. Watch it now!
Posted: August 13, 2012 Filed under: Medical Devices, Uncategorized | Tags: bradycardia, cardiac, cardiac electrophysiology, cardiac techniques, cardiology, conventional devices, defibrillator, eHealthcare, Health 2.0, healthcare applications, heart failure, ICD, Medical Devices, pacemaker, pacemakers, video Leave a commentMeet Mary Soranno, our technical advisor for the UK market presenting all the features of the NayaMed pacemakers & defibrillators. (Better than a long blog post or brochure!).

CARDIOSTIM 2012
Posted: June 26, 2012 Filed under: Congress, Medical Devices | Tags: 2012, 2014, 3D mapping and navigation systems, Cameron Health, cardiac electrophysiology, cardiac techniques, CardioGuide Implant System, Cardiostim, Cardiostim Innovation Award, costs reduction, diagnostics solutions, ICD, leadless pacemaker, Lumax 740 proMRI, Medtronic, NayaMed, Nice, pacemaker, processes simplification, S-ICD, SAS, Sergio Datteri, sleep apnea syndrome, SonR, Sorin Group, St Jude Medical, world congress Leave a comment
Cardiostim 2012, the 18th world congress in cardiac electrophysiology and cardiac techniques has been held in Nice last week and this time more than 5.000 delegates coming from over 100 countries have crowded the congress halls in the Acropolis.
Industry representatives and clinicians had the possibility to meet here in order to discuss on clinical outcomes, new techniques and future technologies.
One of the major innovations presented at the congress had been the 3D mapping and navigation systems dedicated to diagnostics and interventional rhythmology.
These revolutionary tools have been designed to help the implantation of stimulation catheters in CHF patients in order to obtain the best results from the cardiac resynchronization, to simplify the procedures and to reduce the use of fluoroscopy.
In terms of products, Medtronic presented CardioGuide a navigation system for cardiac resynchronization therapy implants. The system is able to generate 3D images of coronary vessels allowing a better road map for finding the best location for the LV lead placement.
St Jude Medical presented MediGuide a mini 3D GPS mapping system able to visualize in real-time the location of a MediGuide enabled device.
A strong focus was given also to the new MRI conditional devices.
Biotronik was present with a big booth entirely dedicated to proMRI devices and in particular to the new Lumax 740 proMRI the first ICD MRI conditional allowing for the first time tachyarrhythmia patients fitted with a device to undergo MR scans.
St. Jude Medical was promoting the Accent MRI family of pacemakers highlighting the availability of a dedicated MRI activator to simplify the device pre-MRI procedures.
Boston scientific showed a panel with a picture of the new pacemaker Ingenio MRI even if this new model MRI compatible seems not yet approved.
A good interest was around new CRT optimization systems with the purpose to improve the response of heart failure patients indicated for CRT.
Sorin presented the new SonR System based on a new hemodynamic sensor mounted in the tip of a dedicated atrial lead (SonRtip) that in combination with the new CRTD device (Paradym RF SonR) is able to provide an automatic weekly optimization.
In the same direction St Jude Medical was promoting the already introduced Quadripolar CRT system applied to the Quadra family of ICDs. This technology enables the physician to find the best pacing site choosing between 10 different LV pacing vectors.
Cameron Health (recently acquired by Boston Scientific) was present at the congress with a booth dedicated to the new S-ICD System, the world’s only ICD that provides reliable defibrillation therapy without transvenous leads. Unlike traditional ICDs that require leads placed in the hearth, this system is the first implantable completely subcutaneously leaving vasculature untouched and eliminating completely complications associated with transvenous leads. In fact both the device and the electrode are implanted just under the skin and outside the ribcage.
In a similar direction Medtronic seems to be working to realize a leadless pacemaker with reduced dimensions that will be implanted directly inside the hearth.
Between other topics, St Jude Medical had a part of the booth dedicated to new Ellipse ICD that with 31cc of volume and 66g of weight seems to be the smallest ICD available on the market (even if not very far from the latest models of Medtronic and Boston Scientific).
Boston Scientific and Sorin were also proposing diagnostics solutions or clinical studies dedicated to the sleep apnea syndrome (SAS), the most widespread sleep breathing disorder commonly associated with increased cardiovascular morbidity and mortality.
The Cardiostim Innovation Award, selected by the congress attendees, honored the S-ICD of Cameron Health, the SonR optimization system of Sorin Group and the CardioGuide Implant System of Medtronic.
NayaMed, the new born cardiac device company with a strong focus on customer optimization and processes simplification, was not present at the congress.
Was it a way to differentiate, again, from all the other companies or just a matter of time to see NayaMed booth at a congress?”
In conclusion, in the beautiful contest of the city of Nice, a very crowded congress with interesting new technologies already available or next to come.
Be ready for the next Cardiostim appointment in June 2014… with NayaMed ?
Here is a quick look of this event :
Sergio Datteri, Independent Medical Device Consultant
Is NayaMed CONNECTIVATE ?
Posted: June 20, 2012 Filed under: NayaMed spirit Leave a comment
Recently I read a booklet from HULT Internal Business School about CONNECTIVATE!
Nothing really revolutionary but a good overview of some companies that success in new ways to connect people, businesses, and other entities to create and capture new value. Somewhere in the book, I came across characteristics to make a company CONNECTIVATE. Immediately, and because human nature is like that, I wondered if NayaMed is using connectivations in dramatically different and powerful ways. Does NayaMed feature an innovation that makes it CONNECTIVATED? As a checklist, I went through the 5 characteristics listed in the book:
- Is available all the time OR everywhere! – Checked, our NayaMed platform is an eCommerce website. By definition it is available all the time and everywhere.
- Improves access to people, products, services or experiences! – Checked, it is indeed the main focus of NayaMed: trying to connect peers; giving easiest access to products; providing web services and new experiences within HCPs organization.
- Creates a fundamental change to a business/industry! – Checked, based on the “emotional” reaction of the market, it is no doubt NayaMed is shaking the rules of the industry of the Medical Devices at least in the way to source our HCPs.
- Has a sustainable business model that makes money! – Checked, of course I am bound by confidentiality but I can tell the business model is sustainable.
- Is the first, or has the most impact compared to similar competitors! – Checked, NayaMed is the first company providing online services for support, procurement and fulfillment through a first-in-the-industry eCommerce/eBusiness website. More than a portal, more than an eOrder process, more than a webshop, much more than a fax machine, NayaMed provides a Customer Commerce platform that helps them to optimize the TCO.
As written in the book: “…all these companies see that the world is flat and the sky is the limit. They project themselves 10x bigger, and they are getting there 10x faster and 10x cheaper…”
Now looking at the customer side, this means raising expectations inevitably. HCPs expect that we know what they like. They expect the best price and a secure transaction of products. Digitalization and homogenization are changing the world. Customers clearly start to see the values they are expecting from companies:
- I want to get what I want or need, when and where I need it
- I want to feel secure and empowered
- I want to be much more confident in the choices and decisions I make
- I want to feel much more connected to people I share with, work with and buy from
At NayaMed, we are getting there, part of our objectives. It can be overnight but only together with our customers. We want to co-create meaningful values. As said by Dr. Stefan Michel (IMD Professor – Strategic Marketing in Action): “What matters is not what we do for our customers, but what really matters is what our customers do with us!” This can’t be wrong.
Thanks to Hitendra Patel, Ronald Jonash, Steve Wyatt and Victor Fernandes for their inspired book.
Frédéric Briguet
Head of eBusiness and Marketing
NayaMed



{kind=link}